What is COVID-CAT (COVID-19 Capacity Analysis Tool)?
COVID-CAT is a tool for hospital and emergency department (ED) managers, physicians, and health care workers to quickly convert predictions of future COVID-19 patient arrivals into predictions of future COVID-19 census levels in the ED, main hospital, and the ICU. The software provided on this page is the latest version, which we have been developing here at UNC since mid-March 2020.
The underlying mathematical model does not assume anything specific to the characteristics of COVID-19 patients (except for user specified settings related to patients’ length-of-stay) but the flow of COVID-19 patients in the ED to the main hospital and the ICU, their relatively isolated treatment, at least as is practiced at UNC ED and hospitals, makes this model and the tool particularly useful for predicting bed capacity demands for COVID-19 patients. The goal is to provide rough and quick projections to carry out what-if analyses relying on few inputs, which can be easily obtained by a physician or a hospital manager. The tool provides healthcare workers and managers a sense of
- when the bed needs will surge if at all,
- the magnitude of any predicted surge,
- what bed capacities will be needed to meet patient demand.
Hospital and ICU analyses are run on a daily time scale while the ED analysis is run on an hourly time scale.
The required inputs include
for ED capacity analysis:
- mean and standard deviation of ED length-of-stay for COVID-19 patients,
- current ED census (current number of ED beds occupied by COVID-19 patients),
- daily arrival predictions of suspected or confirmed COVID-19 cases (also needed for ICU and hospital capacity analysis),
- hourly arrival percentages (specifying the percentages of daily arrival total that will arrive over each hour of a day, altogether 24 numbers adding up to 1);
for hospital capacity analysis:
- mean and standard deviation of hospital length-of-stay for COVID-19 patients,
- current hospital census (current number of hospital beds occupied by COVID-19 patients),
- daily arrival predictions of suspected or confirmed COVID-19 cases (also needed for ICU and hospital capacity analysis),
- the percentage hospitalized as confirmed COVID-19 cases among the patients who arrive as suspected or confirmed COVID-19 cases;
for ICU analysis:
- mean and standard deviation of ICU length of stay for COVID-19 patients,
- current ICU census (current number of ICU beds occupied by COVID-19 patients),
- daily arrival predictions of suspected or confirmed COVID-19 cases (also needed for ICU and hospital capacity analysis),
- the percentage who needs ICU care among the patients who arrive as suspected or confirmed COVID-19 cases.
Daily arrival predictions and hourly arrival percentages are stored in two txt files (ArrivalRate.txt and HourlyPattern.txt), which the user can update as the predictions for new cases change. All other inputs are directly entered by the user in the boxes that appear when the tool is run.
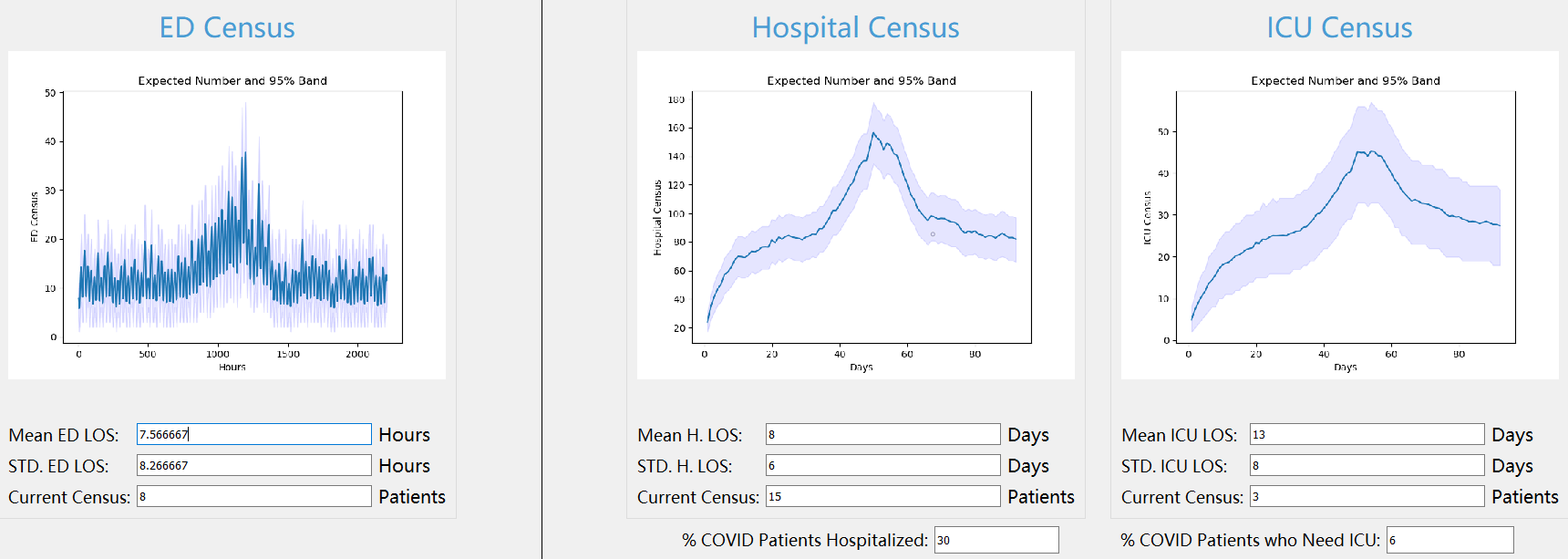
ED, Hospital, and ICU analyses are run separately. As long as valid input is provided, clicking the Run button for any type of analysis will run the tool and generate a new plot and a report. The plot will show the projected mean, the 5% quantile, and the 95% quantile for the approximate distribution obtained for different times in the future. The tool also generates a report, where an approximation for the probability of exceeding a given threshold within a certain period of time is provided.
Below is a screen-shot of the COVID-CAT output screen when it is run with hypothetical data and estimates. To download COVID-CAT as a standalone application or more details on the methodology see below. Work is under way to make COVID-CAT an online, web-based application.
Resources
Methodology
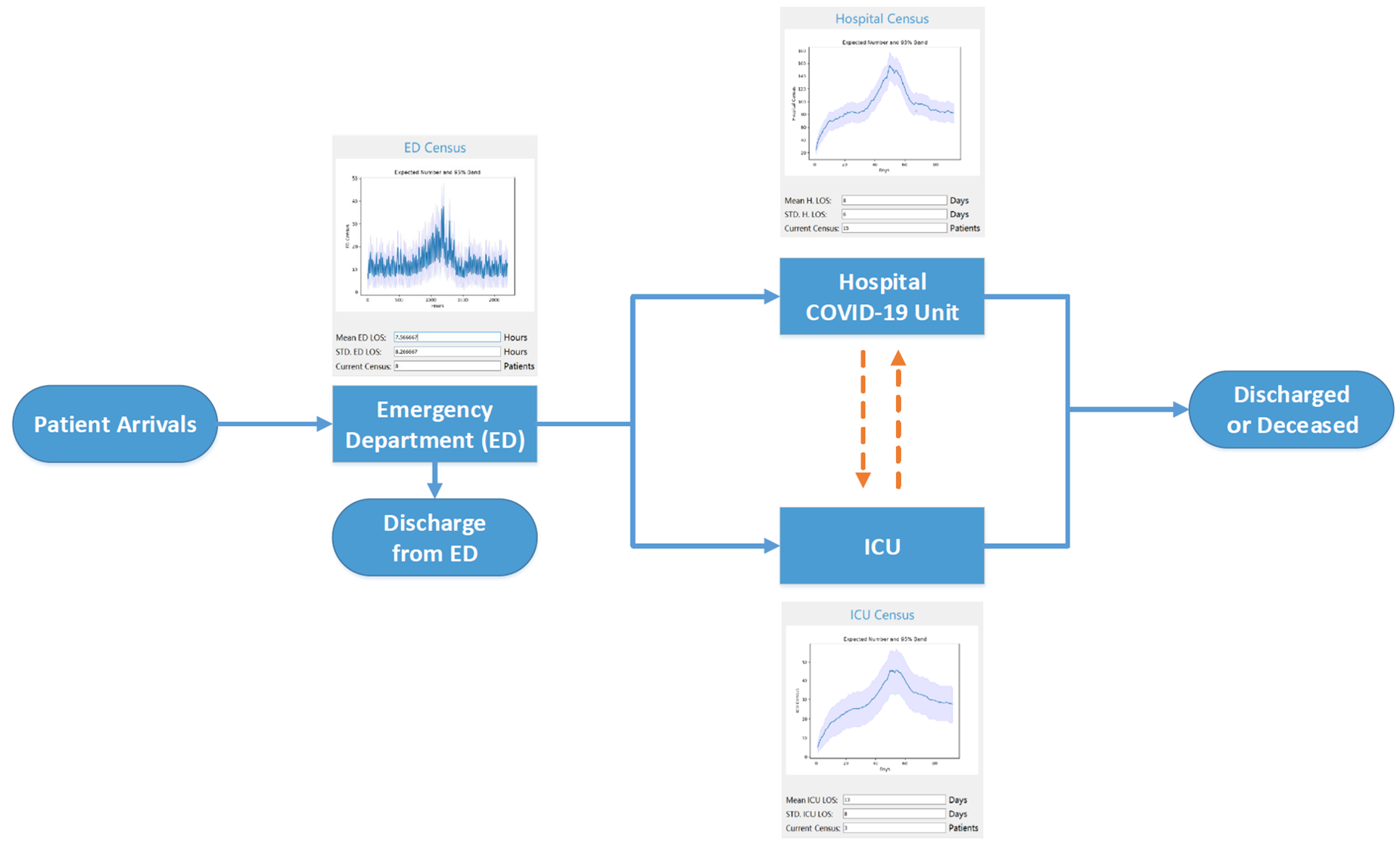
Below is a visual representation of what the mathematical model assumes regarding patient flow. COVID-19 suspected or confirmed patients arrive at the ED. After their stay in the ED is complete, they are either discharged from the ED, admitted to the main hospital COVID-19 unit, or admitted directly to the ICU. Patients who are admitted to the COVID-19 unit initially may later be transferred to the ICU if their condition deteriorates; similarly, patients who are first admitted to the ICU may be transferred to the COVID-19 unit in the hospital if their condition improves. The user may set the percentages of admission to the hospital and the ICU so as to account for these possibilities. However, it is important to note that the mathematical model assumes that patients start occupying a bed in the hospital and/or the ICU right after the patient’s stay in the ED is over and therefore the model would be biased towards capturing the bed demand in the hospital and the ICU slightly early.
The methodology behind COVID-CAT is based on known results from queueing theory, more specifically the analysis of the 
One implicit assumption of the model is that all patients who arrive at the ED are admitted, and all patients who need hospitalization and/or ICU are also admitted. This means that the model assumes that there are no limits on the numbers of COVID-19 patients the ED, the hospital, and the ICU can have at any point in time. Therefore, the predictions made by COVID-CAT should be interpreted as bed capacities that would be needed to fully meet the patient demand at different points in time in the future. They should NOT be interpreted as what the actual census levels will be as those levels would be ED and hospital specific depending on the number of beds available as well as the policies the ED and the hospital would adopt to deal with the excess demand. By not making specific assumptions on bed capacities as well as such policy choices, we aim to make the tool useful not only for UNC but other EDs and hospitals as well.
Future Directions
- Integrating an epidemic model into the tool to predict future trajectories.
- Developing an online version of COVID-CAT (managed by Yunying and Yichen).
Leave a Reply